
Marijuana Use in Older Drivers in Colorado: A LongROAD Study
This research brief describes marijuana use and its relationship to self-reported driving outcomes among older drivers using baseline data from the Colorado cohort of the LongROAD study.
April 2018
Suggested Citation
For media inquiries, contact:
Tamra Johnson
202-942-2079
TRJohnson@national.aaa.com
Abstract
This research brief used baseline data from the Longitudinal Research on Aging Drivers (LongROAD) study to characterize marijuana use and its relation to self-reported driving outcomes in older adult drivers. Recent U.S. studies have demonstrated significant increases in marijuana use among adults ages 65+ over the past decade (Han et al., 2016; Hasin et al., 2015; Salas-Wright et al., 2017). Here, we describe marijuana use among 598 drivers ages 65-79 in Colorado and its relationship to risky driving behaviors and adverse outcomes. Of 54 participants (9.0%) who reported marijuana use in the past year, one-third used it at least weekly. The rate of past-year marijuana use in the Colorado LongROAD cohort was substantially higher than in recently reported nationally representative surveys, which may be due to national trends showing increasing use in older adults (Han et al., 2016) and to Colorado’s recent legalization of recreational marijuana (National Conference of State Legislatures, 2017). In the Colorado LongROAD cohort, older drivers rarely reported marijuana use within one hour of driving. However, past-year marijuana users were four times as likely to report having driven when they may have been over the legal blood-alcohol limit compared with those who had not used marijuana in the past year. Despite potential risks from both marijuana use and increased driving after drinking, there was no increase in the likelihood of having a crash or police action (e.g., being pulled over) in the past year in this sample of older drivers who reported using marijuana in the past year.
Methods
This study used baseline data from the LongROAD study (Li et al., 2017). LongROAD is a multisite (Ann Arbor, Michigan; Baltimore, Maryland; Cooperstown, New York; Denver, Colorado; and San Diego, California) prospective cohort study designed to collect data on the medical, behavioral, environmental and vehicle technological factors associated with safe driving in older adults. Study participants were drivers ages 65-79 at enrollment who had a valid driver’s license, drove on average at least once a week using a vehicle of model year 1996 or newer and had no significant cognitive impairment. For this study, the sample was limited to participants from the Colorado study site, which is the only site that collected data on marijuana use at baseline. Colorado passed a medical marijuana law in 2000 and subsequently amended the law in 2012 to allow recreational use of marijuana. Data were collected from August 2015 through March 2017.
Colorado participants were asked if they had ever used cannabis, marijuana or hash (referred to hereafter as “marijuana”); how many times, if any, they had used marijuana during the past 12 months; if they had driven a motor vehicle within one hour of using marijuana in the past year and, if so, how many times in the past 30 days they had driven within one hour of using marijuana. Participants who reported using marijuana one or more times within the past 12 months were considered to be past-year “marijuana users.” We compared them with participants who reported not using marijuana in the 12 months before the baseline visit (“nonusers”). Participants were also asked how often they drove even though they may have been over the legal blood-alcohol limit (“drinking and driving”), and if they had any crashes or police actions (i.e., being pulled over, being ticketed other than for parking violations) in the past year.
Demographic characteristics assessed included age, gender, race, ethnicity, education, income, employment, marital status and work for pay, categorized as shown in Table 1. Health-related characteristics examined included alcohol use in the past three months, having four or more alcoholic drinks on one occasion in the past three months, health-care utilization (self-reported emergency department visits or hospitalizations; health conditions (categorized based on organ system, excluding conditions affecting fewer than 5% of participants); Patient-Reported Outcomes Measurement Information System (PROMIS) measures of social, mental and cognitive health; and cognitive function based on the Telephone Interview for Cognitive Status (TICS) (with lower scores indicating poorer cognitive function). PROMIS measures were scored using PROMIS (HealthMeasures, 2017) and American Psychiatric Association guidelines for the specific PROMIS survey items (American Psychiatric Association, 2013), with higher scores indicating more of the symptoms or condition.
For analysis, we examined distributions of driver characteristics among past-year marijuana users and nonusers, calculating crude (unadjusted) prevalence ratios (PRs), 95% confidence intervals (CI) and p-values, using log-binomial regression, for past-year marijuana use. We estimated adjusted odds ratios (ORs) and corresponding 95% CIs for associations between past-year marijuana use versus nonuse and the adverse driving outcomes of (a) drinking and driving and (b) self-reported crashes/police actions, using logistic regression models. We assessed sociodemographic and health variables as potential confounders for each of these adverse driving outcomes. Final multivariable models included only variables that were associated with both the selected outcome and marijuana use in our data and that changed the effect estimates by 10% or more. Results are reported as odds ratios at an alpha level of 0.05 for testing statistical significance.
Results
The Colorado site enrolled 600 participants for the LongROAD study, of whom the majority were married, retired, of white race and non-Hispanic ethnicity; earned at least $80,000 per year and had at least a bachelor’s degree. Fifty-one percent were female and the mean age was 70.6 years (sd=4.1).
Among Colorado participants, 598 (99.7%) provided data on marijuana use and 244 (40.7%) reported having used marijuana at some point in their life. Fifty-four participants (9.0%) reported use in the past year, of whom 27 (50.0%) used marijuana less than once a month, nine (16.7%) one to three times per month, 11 (20.4%) one to five times per week, and seven (13.0%) more than once per day. Only five participants (0.8%) reported having used marijuana within one hour of driving in the past year, while three (0.5%) had used it within one hour of driving in the past 30 days.
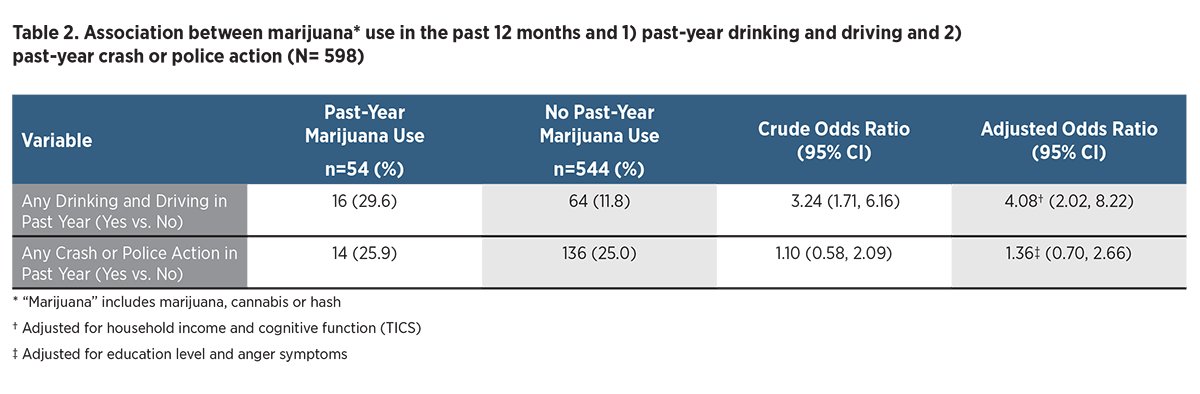
Table 1 shows demographic and health characteristics of older drivers who had and had not used marijuana within the past year. Compared with older drivers who had not used marijuana in the past year, past-year marijuana users were younger and less highly educated and had a lower household income but otherwise had similar sociodemographic characteristics. Past-year marijuana users were more likely to report alcohol use in the past three months and to have been diagnosed with a mental health condition (e.g., depression or anxiety disorder). None of the past-year users had been diagnosed with substance abuse/alcohol dependency. Distributions of other h ealth conditions were similar between groups. All measures of mental, emotional, social and cognitive health, including depression, anxiety, anger, social isolation, lack of emotional support, concerns about cognitive health and measured cognitive status were worse in past-year marijuana users. For example, they were about six times as likely to report moderate to severe anxiety and nearly twice as likely as nonusers to report having no to slight emotional support (Table 1).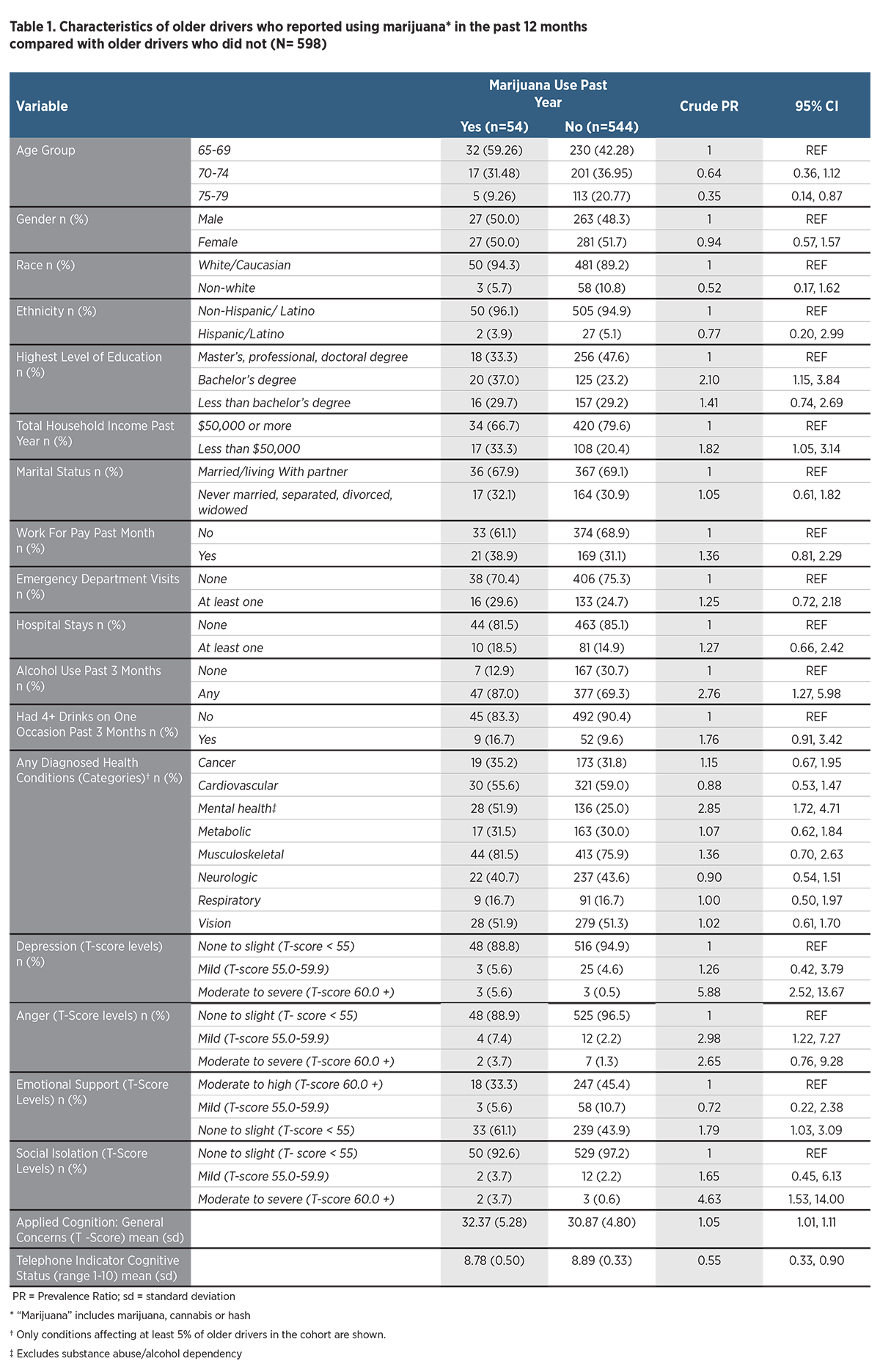 Table 2 shows the relationship between past-year marijuana use and adverse driving outcomes. Compared with older drivers who had not used marijuana in the past year, past-year marijuana users were more likely to report drinking and driving (OR = 3.56; 95% CI: 1.93, 6.55). The odds of self-reported drinking and driving among past-year marijuana users were four times as high as among nonusers after accounting for other differences between groups (adjusted OR=4.08; 95% CI: 2.02, 8.22). However, marijuana use in the past year was not associated with significantly increased odds of self-reported involvement in a crash or police citation in the past year compared with nonusers after accounting for other differences between groups (adjusted OR=1.36; 95% CI: 0.70, 2.66).
Table 2 shows the relationship between past-year marijuana use and adverse driving outcomes. Compared with older drivers who had not used marijuana in the past year, past-year marijuana users were more likely to report drinking and driving (OR = 3.56; 95% CI: 1.93, 6.55). The odds of self-reported drinking and driving among past-year marijuana users were four times as high as among nonusers after accounting for other differences between groups (adjusted OR=4.08; 95% CI: 2.02, 8.22). However, marijuana use in the past year was not associated with significantly increased odds of self-reported involvement in a crash or police citation in the past year compared with nonusers after accounting for other differences between groups (adjusted OR=1.36; 95% CI: 0.70, 2.66).
Discussion
Lifetime marijuana use was common among this group of Colorado drivers ages 65-79, but only 9% reported having used marijuana in the past year, and very few reported using marijuana within one hour of driving. Among past-year users, half used marijuana less than once a month, but one-third used it at least once a week.
Prevalence of past-year marijuana use among older drivers in the LongROAD cohort was substantially higher than in recently reported nationally representative surveys. For example, Choi et al. (2016), in the National Epidemiologic Survey on Alcohol and Related Conditions, found only 1.65% of respondents ages 65+ reported past-year use in 2012-2013. In the National Survey on Drug Use and Health, past-year use in persons ages 65+ was reported to be 1.4% in 2012-2013 (Han et al., 2016) and 2.1% in 2014 (Salas-Wright et al., 2017). Salas-Wright et al. (2017) reported that marijuana users ages 65+ were more likely to be male, African-American, and divorced or separated, and less likely to have no more than a high school degree relative to college graduates (Salas-Wright et al., 2017). In our sample, 89% of participants were white, 63% were married and 82% had at least a college degree; hence, a lower rather than higher rate of marijuana use would have been expected based on risk factors reported by Salas-Wright et al. (2017). Several factors could explain the higher rate of use in our sample. We collected our data more recently than these other studies. Han et al. (2016) reported a 250% relative increase in cannabis use between 2006/2007 and 2012/2013, and that upward trend is likely to have continued. Further, Colorado is one of the few U.S. states to have legalized recreational marijuana (National Conference of State Legislatures, 2017). This may have resulted either in more older adults in Colorado using marijuana, or a greater proportion being willing to report their use, than those living in other states.
Past-year marijuana users demonstrated a constellation of mental health-related diagnoses and problems affecting nearly every aspect of mental, social and emotional health assessed. Perhaps surprisingly, none of the past-year marijuana users in our study reported having been diagnosed with a substance abuse disorder or alcohol dependency, whereas having other mental health conditions among marijuana users was nearly three times as common as among nonusers. Ours is not the first study to report higher rates of mental health conditions or symptoms among older marijuana users. Choi et al. (2016), in a nationally representative sample of adults ages 50+, similarly found high rates of mental health conditions, as well as more life stressors and lower perceived social support, among marijuana users. Han et al. (2016) found that, among persons ages 50+, past-year use of tobacco, alcohol or illicit drugs increased the odds for reporting past-year cannabis use, as did a history of mental health treatment. Using the same survey, but limited to those ages 65+, Salas-Wright et al. (2017) found that past-year marijuana users were more likely to binge-drink alcohol, use illicit drugs, sell drugs, steal and have been arrested. They were also three times as likely to report past-year anxiety and nearly twice as likely to report depression.
Less than 1% of older drivers in our study reported having driven within one hour of using marijuana at any time in the past year. To our knowledge, there are no other U.S. data reporting driving behavior among older adults after marijuana use, and further evaluation is warranted. There are few data with which to compare these findings. Alvarez et al. (2007) surveyed people selected from a representative sample of households in two regions of Spain. Among persons ages 50-70, an estimated 0% reported driving under the influence of cannabis, although 7% reported being a passenger in a vehicle driven by someone under the influence (on a mean of two days in the past year). Both Alvarez et al. (2007) and our study thus suggest that self-reported driving while impaired with marijuana is rare among older drivers.
Marijuana has been shown to impair cognition (e.g., attention, vigilance, perception of speed) and driving performance (Sewell et al., 2009; Kelly et al., 2004). In general, the higher the estimated concentration of tetrahydrocannabinol (THC) in the blood, the greater the driving impairment, although more frequent users show less impairment than infrequent users at the same concentration, presumably because of physiological tolerance or learned compensatory behavior. However, tolerance in older adults specifically has not been examined and may apply differently than in young or middle-aged adults. Reviews of epidemiologic studies of crash risk have shown conflicting results, with some showing increased risk and others no increased risk with marijuana use (Asbridge et al., 2012; Compton & Berning, 2015; Elvik, 2013; Kelly et al., 2004; Li et al., 2012; Sewell et al., 2009), although none of the included studies focused solely or primarily on older adults. Finally, an analysis of Fatality Analysis Reporting System (FARS) data from 1992-2009 demonstrated no increase in prevalence of cannabinoids among drivers involved in fatal crashes or in fatally injured drivers in Colorado after medical marijuana laws were passed, once frequency of testing after crashes and national trends in use were taken into account (Masten et al., 2013). In our study, past-year marijuana use was not associated with any increase in risk of having a crash or being pulled over or ticketed by police. The lack of association with crash risk is consistent with some previous studies but may also reflect the small number of marijuana users examined or the fact that older drivers in the LongROAD cohort rarely reported driving immediately after marijuana use.
Of concern, marijuana users were significantly more likely to report driving when they may be over the legal blood-alcohol limit. Salas-Wright et al. (2017) similarly found significantly high risk for driving under the influence of alcohol among past-year marijuana users compared with nonusers. Even though marijuana users may not report driving while impaired by marijuana, such use may be a marker for older adults who are at greater risk for driving while impaired by alcohol and thus for alcohol-related crashes and crash fatalities. Further, laboratory study suggests that simultaneous use of alcohol and cannabis produces significantly higher blood concentrations of cannabis’s main psychoactive constituent, Δ9-tetrahydrocannabinol (THC), than cannabis use alone (Hartman et al., 2015). Additional study is needed regarding driving behavior related to use of marijuana and alcohol as well as medications that can affect cognition such as opioids and benzodiazepines.
The findings reported here were based on a sample of affluent, highly educated older drivers living in Colorado; these results may not be generalizable to other populations or locales. Further, results were based solely on self-reporting. In addition, the number of past-year marijuana users was relatively small, limiting the study’s power to identify small differences between past-year users and nonusers. Despite these limitations, the study adds important new information to the very limited data available on marijuana use among older drivers and its relationship to driving. In future years, multiple sites participating in the LongROAD study plan to collect data on marijuana use, which will provide a larger, more diverse sample from which to draw conclusions about its effect on driving behavior and driving safety.
References
Alvarez, F. J., Fierro, I., Del Rio, M. C. (2007). Cannabis and driving: results from a general population survey. Forensic Sci Int, 170:111-116.
American Psychiatric Association. (2013) Online Assessment Measures. Retrieved from https://www.psychiatry.org/psychiatrists/practice/dsm/educational-resources/assessment-measures.
Asbridge, M., Hayden, J. A., Cartwright, J. L. (2012). Acute cannabis consumption and motor vehicle collision risk: systematic review of observational studies and meta-analysis. Bmj, 344(2). doi:10.1136/bmj.e536.
Choi, N. G., Dinitto, D. M., Marti, C. (2016). Older marijuana users: Life stressors and perceived social support. Drug and Alcohol Dependence, 169:56-63. doi:10.1016/j.drugalcdep.2016.10.012.
Compton, R. P. & Berning, A. (2015, February). Drug and alcohol crash risk. (Traffic Safety Facts Research Note. DOT HS 812 117). Washington, DC: National Highway Traffic Safety Administration.
Elvik, R. (2013). Risk of road accident associated with the use of drugs: A systematic review and meta-analysis of evidence from epidemiological studies. Accident Analysis & Prevention, 60:254-67.
Han, B. H., Sherman, S., Mauro, P. M., Martins, S. S., Rotenberg, J., Palamar, J. (2016). Demographic trends among bolder cannabis users in the United States, 2006–13. Addiction, 112:516-525. doi:10.1111.
Hasin, D. S., Saha, T. D., Kerridge, B. T., et al. (2015). Prevalence of Marijuana Use Disorders in the United States Between 2001-2002 and 2012-2013. JAMA Psychiatry, 72(12):1235. doi:10.1001/jamapsychiatry.2015.1858.
Hartman, R. L., Brown, T. L., Milavetz, G., Spurgin, A., Gorelick, D. A., Gaffney, G., Huestis, M. A. (2015). Controlled cannabis vaporizer administration: blood and plasma cannabinoids with and without alcohol. Clinical Chemistry, 61(6):850-69. doi: 10.1373/clinchem.2015.238287. Epub 2015 May 27.
HealthMeasures. PROMIS. Evanston: Northwestern University. (2017). Retrieved from: http://www.healthmeasures.net/score-and-interpret/interpret-scores/promis
Kelly, E., Darke, S., Ross, J. (2004). A review of drug use and driving: epidemiology, impairment, risk factors and risk perceptions. Drug and Alcohol Review, 23(3):319-344. doi:10.1080/09595230412331289482.
Li, G., Eby, D., Santos, R., Mielenz, T. J., Molnar, L. J., Strogatz, D., Betz, M., DiGuiseppi, C., Ryan, L. H., Jones, V., Pitts, S. I., Hill, L. L., DiMaggio, C. J., LeBlanc, D., Andrews, H. F., the LongROAD Research Team. (2017). Longitudinal research on aging drivers (LongROAD): study design and methods. Innovation in Aging, 1(Suppl_1), 1262-1263. doi:10.1093/geroni/igx004.4597
Li, M. C., Brady, J. E., DiMaggio, C. J., Lusardi, A. R., Tzong, K. Y., Li, G. (2012). Marijuana Use and Motor Vehicle Crashes. Epidemiologic Reviews, 34(1):65-72. doi:10.1093/epirev/mxr017.
Masten, S. V., Guenzburger, G. V. (2014). Changes in driver cannabinoid prevalence in 12 U.S. states after implementing medical marijuana laws. Journal of Safety Research, 50:35-52. doi:10.1016/j.jsr.2014.03.009.
National Conference of State Legislatures. State Medical Marijuana Laws. (2017) http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx, accessed 8/30/2017.
Salas-Wright, C. P., Vaughn, M. G., Cummings-Vaughn, L. A., et al. (2017). Trends and correlates of marijuana use among late middle-aged and older adults in the United States, 2002–2014. Drug and Alcohol Dependence, 171:97-106. doi:10.1016/j.drugalcdep.2016.11.031.
Sewell, R. A., Poling, J., Sofuoglu, M. (2009). The Effect of Cannabis Compared with Alcohol on Driving. American Journal on Addictions, 18(3):185-193. doi:10.1080/10550490902786934.
Suggested Citation
For media inquiries, contact:
Tamra Johnson
202-942-2079
TRJohnson@national.aaa.com