This research brief utilized data from the Longitudinal Research on Aging Drivers (LongROAD) study to examine the effect of lifetime musculoskeletal condition diagnoses on driving reduction in the past year in an older driver population. Musculoskeletal conditions—such as arthritis, joint pain, and peripheral neuropathies—have been known to impact driving habits, increasing the need for driving restrictions and modifications (Pomidor, 2016). Here, we examined older drivers with musculoskeletal diagnoses to examine reduced driving from those diagnoses. We found that women were slightly more likely to have a musculoskeletal diagnosis and twice as likely to reduce driving as a result. The highest rates of driving reduction were due to hip and knee replacements, while the greatest number of driving reductions were due to joint pain and swelling and arthritis other than rheumatoid arthritis.
Methods
This study utilized cross-sectional, baseline data from the AAA Foundation LongROAD study, a longitudinal study on aging drivers. LongROAD is a multisite (California, Colorado, Maryland, Michigan, and New York) prospective cohort study designed to collect data on the medical, behavioral, environmental, and vehicle technological factors influencing older adults in driving safely. Participants were eligible if they were 65-79 years old, possessed a valid driver’s license, drove at least once per week on average, and had no significant cognitive impairment.
LongROAD collects self-reported and objectively measured information on health status and driving behaviors. Questions analyzed for this study included those regarding health condition diagnoses and driving reduction. Health status questions were based on the National Health and Aging Trend Study questionnaire. Participants were first asked whether they reduced driving because of any health conditions at all in the past 12 months. Then they were asked if they had ever had any of 55 health conditions in their lifetime. For each diagnosis, participants who had reported decreasing driving for any condition were asked if they had reduced driving as a result. Among the 109 total diagnosis categories reported, 20 were musculoskeletal health conditions (i.e. arthritis, joint replacement, osteoporosis, etc.). This analysis examines participants who self-reported having at least one of these musculoskeletal conditions.
Results
Demographics
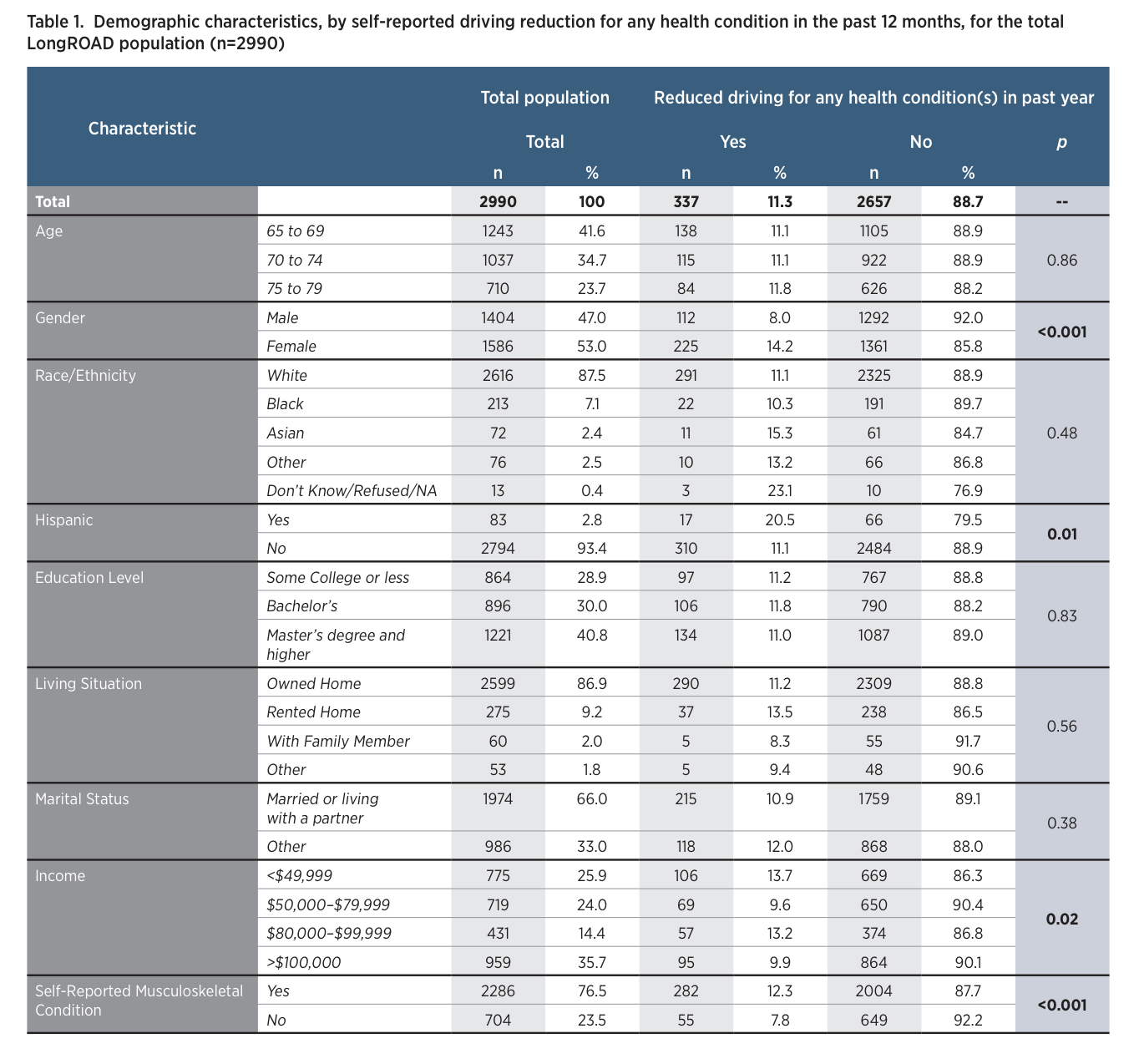
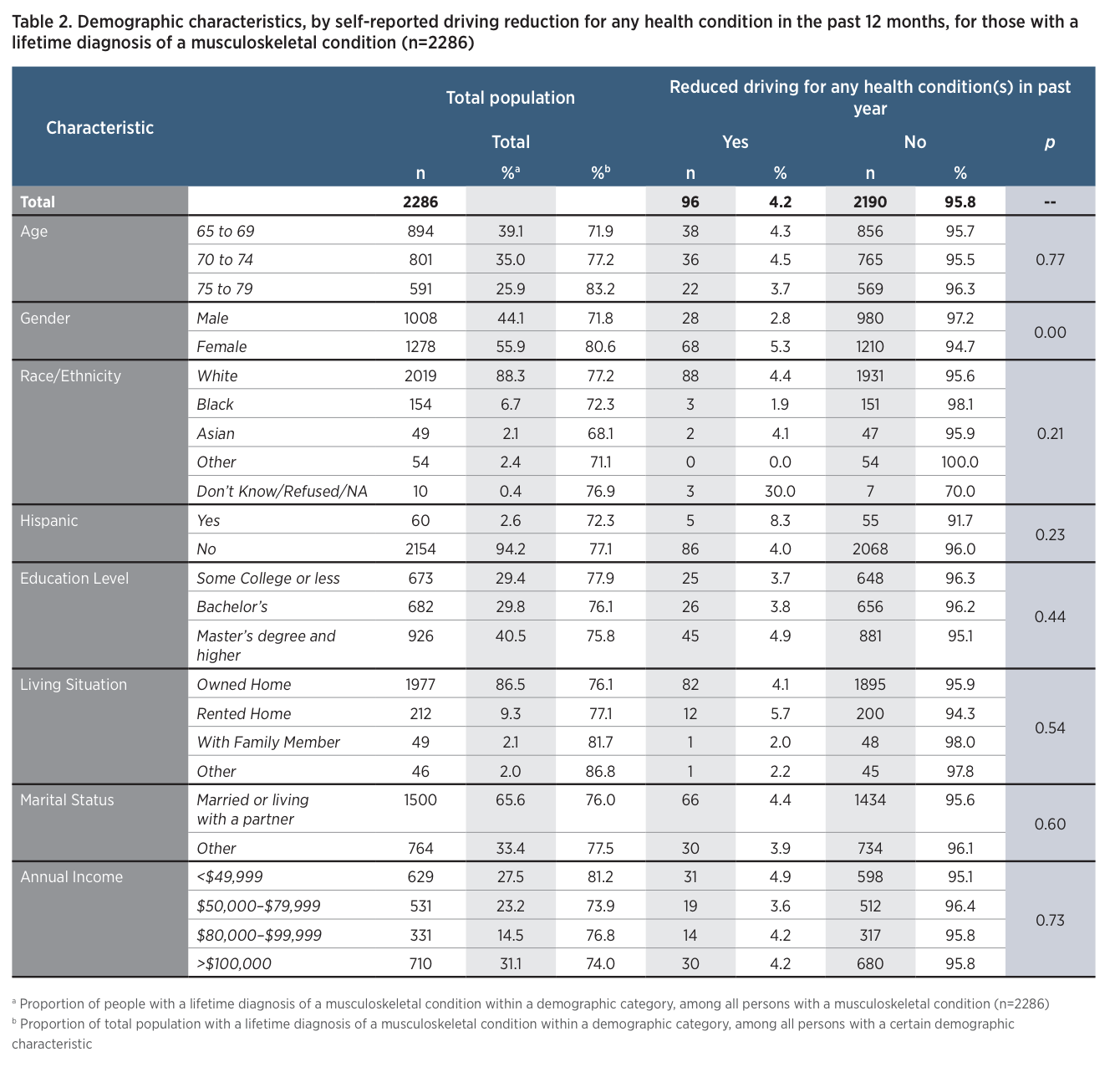
Overall, among the 2,990 older drivers in the LongROAD study, 2,286 (77%) reported having a musculoskeletal health condition during their lifetime (Table 1). When examining demographic characteristics (Table 2), the number of musculoskeletal diagnoses increased with age: 72% of those aged 65-69 years, 77% of those aged 70-74, and 83% of those aged 75-79 had experienced a musculoskeletal condition diagnosis during their lifetime. Major differences in musculoskeletal diagnosis did not exist based on race, Hispanic ethnicity, or marital status. Those with lower levels of education (less than a bachelor’s degree) or who did not own their own home were more likely to have had a musculoskeletal condition (Table 2). Musculoskeletal conditions were also more common among those with an annual income of less than $49,999. Older adults who reported having a musculoskeletal diagnosis during their lifetime were more likely to report driving reduction for any health condition in the past year (12.3% versus 7.8%; Table 1). Of the 337 drivers in the LongROAD cohort who reduced driving because of a health condition, 96 (29%) did so due to a musculoskeletal condition. Overall, 4.2% of those with a lifetime musculoskeletal condition reported having reduced driving in the past year because of this diagnosis (Table 2).
Gender
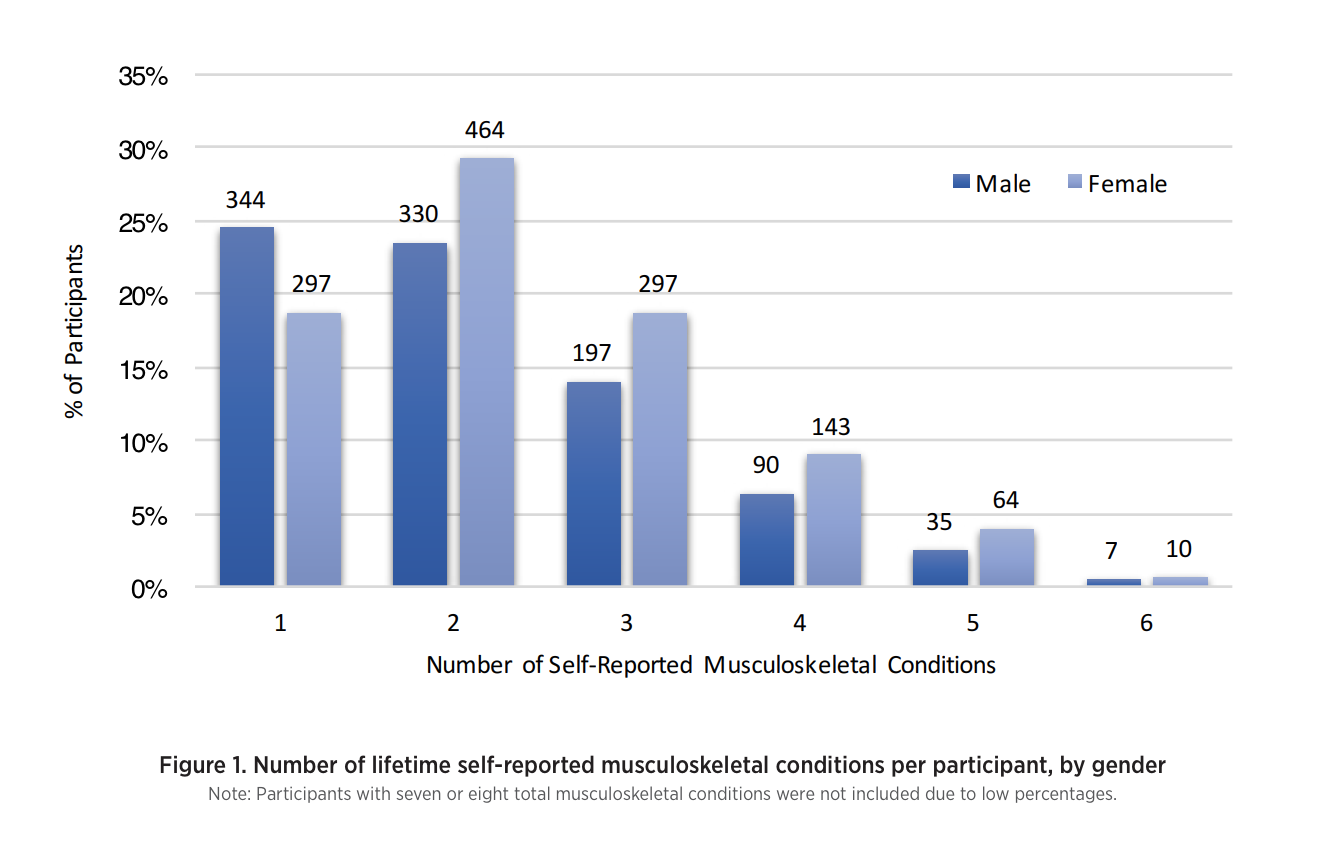
A greater proportion of women, compared with men, reported having had at least one musculoskeletal condition in their lifetime (81% versus 72%; Table 2) and were significantly more likely to report musculoskeletal diagnoses, on average, than men as shown in Figure 1 (mean: 2.42 vs 2.19). Females with a musculoskeletal condition were almost twice as likely to reduce driving in the past 12 months when compared with males with a musculoskeletal condition (5.3% versus 2.8%; Table 2).
Specific Musculoskeletal Conditions
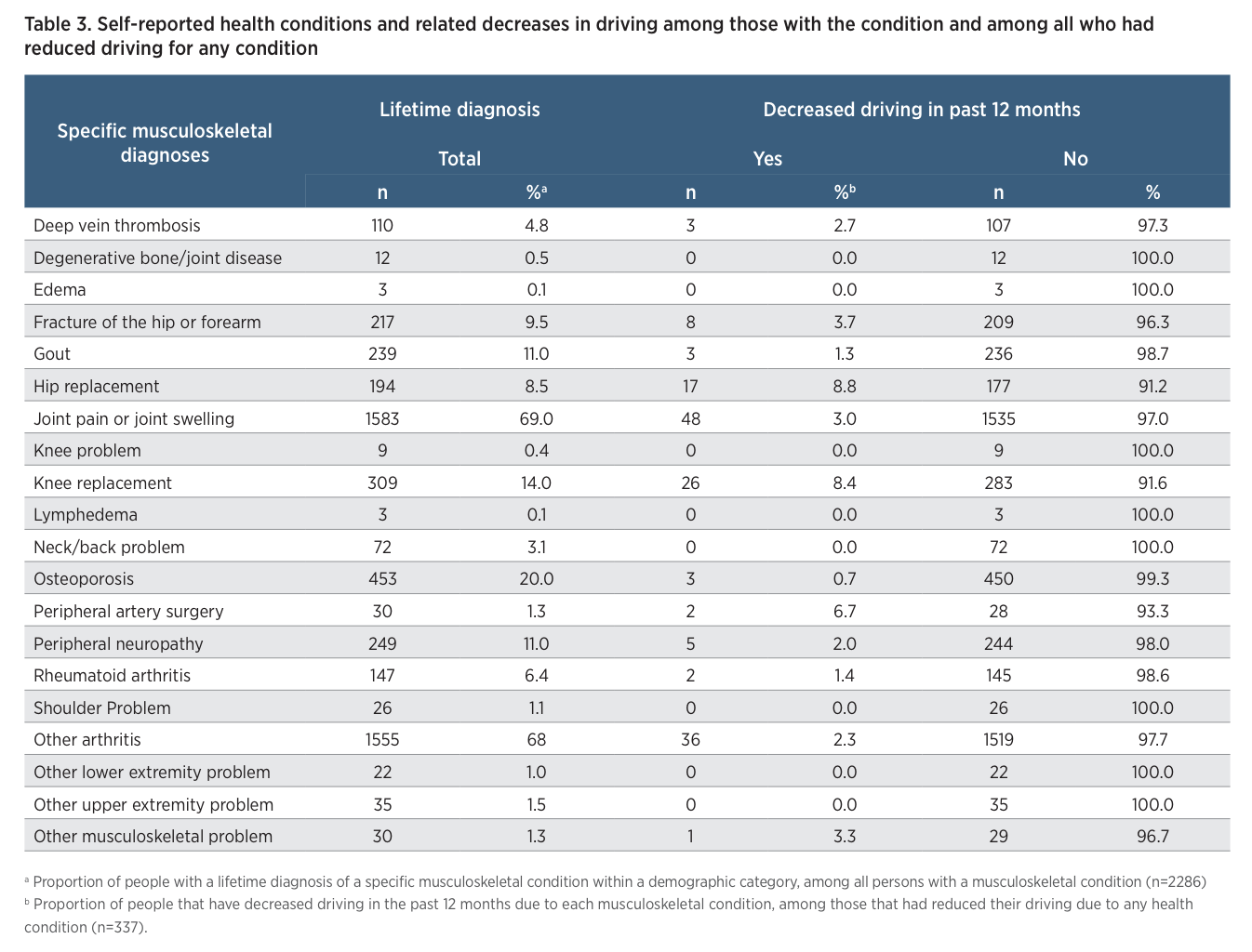
Among those with a lifetime history of at least one musculoskeletal condition, the most common conditions reported were joint pain and swelling (69%) and arthritis other than rheumatoid arthritis (68%) (Table 3). These conditions were also associated with the greatest numbers of driving reductions, with 48 participants reducing driving because of joint pain and swelling and 36 participants doing so because of arthritis other than rheumatoid arthritis. Because these conditions were common, they resulted in low overall rates of related driving reduction (3% and 2.3%, respectively). With regards to the highest rates of driving reduction due to a specific condition, hip replacement caused 8.8% (17 of 194) of older drivers to decrease driving in the past year, while knee replacement caused 8.4% (26 of 309) of older drivers to do so.
Discussion
A majority of the LongROAD cohort self-reported having experienced at least one musculoskeletal condition in their lifetime, and those with these conditions had reduced their driving notably. For those with musculoskeletal diagnoses, joint pain and swelling and arthritis other than rheumatoid arthritis caused large numbers of participants to reduce driving in the past year, while musculoskeletal surgeries such as hip replacement and knee replacement caused high rates of driving reduction. Additionally, women were more likely than men to report decreased driving because of musculoskeletal conditions. As found in prior research, musculoskeletal conditions (e.g., arthritis), symptoms (joint pain and swelling) and surgeries (hip and knee replacements) were all associated with driving reduction in this large cohort of older drivers (Braitman & McCartt, 2008; Charlton et al., 2006). Some of these conditions are potentially progressive and chronic, while others are temporary; for example, six weeks of driving reduction is required when recovering from joint replacement surgery (Braitman & McCartt, 2008; Ragland, Satariano, & MacLeod, 2004). One potential confounder in this relationship may be the effect on driving ability of pain medications taken for musculoskeletal conditions. Not only do these medications cause side effects such as dizziness that may cause older adults to decrease driving, this cohort may also be more susceptible to such side effects compared with younger populations (Ray, Gurwitz, Decker, & Kennedy, 1992; Wang & Carr, 2004).
Participant gender greatly influenced the number of people who self-reported driving reduction due to lifetime musculoskeletal condition diagnoses in this older driver cohort. Females were more likely to have a musculoskeletal diagnosis and to consequently reduce driving compared with their male counterparts. This may be because women are more likely to see healthcare providers about potential health problems (and thereby receive a diagnosis) and because they are more likely to decrease their driving, in general, with increasing age (Choi, Adams, & Kahana, 2013; Xu & Borders, 2003). Confidence may also affect driving reduction in older adults of both genders. Low confidence in driving ability, coupled with musculoskeletal condition diagnosis, might cause premature driving reduction for women. Conversely, overconfidence in driving ability and pressure to maintain a traditional provider role might cause men to continue driving (Brabyn, Schneck, Lott, & Haegerström-Portnoy, 2005; Charlton et al., 2006; Marottoli et al., 1993). Because premature driving reduction has been associated with decreased quality of life, clinicians, family members, and traffic safety professionals should account for the role of gender and personality in the process of counseling older adults on driving reduction (Chihuri et al., 2015).
The main limitation in this study is that baseline data only considered lifetime prevalence of musculoskeletal condition diagnosis (i.e., those who ever had a musculoskeletal condition in their lifetime) and driving reduction based on health conditions that occurred more than a year in the past could not be quantified. We also did not have detailed information about the severity of conditions or the specific physical locations of certain conditions (e.g., left versus right leg), which are factors that may play a part in affecting driving ability. Despite these limitations, this study confirms that some musculoskeletal conditions may cause the older population to decrease driving. Future work with the LongROAD cohort will consider the role of medication on driving reduction and consider how other factors may play a part in reducing older adult mobility.
Simple adjustments to vehicles might overcome some limitations caused by musculoskeletal conditions. For example, thick steering wheels and keyless entry could alleviate the debilitating effects of conditions such as arthritis (https://seniordriving.aaa. com/maintain-mobility-independence/car-buying-maintenance-assistive-accessories/smartfeatures/), and larger mirrors and assistive devices on doors or seats can mitigate limited neck mobility or difficulty entering or exiting the vehicle. Many of these devices can be added to existing vehicles at a low cost, and occupational therapists can assist in training with more complicated devices such as hand controls. CarFit, an educational program through which community workers help older adults to evaluate how well their car fits their physical abilities and needs (https://seniordriving.aaa.com/maintain-mobility-independence/ car-buying-maintenance-assistive-accessories/carfit/), also offers promise as it helps older drivers optimize seat and mirror positioning. With appropriate diagnosis and treatment of musculoskeletal conditions, and with appropriate attention to vehicle modifications, healthcare providers, family, and community groups can work together to help keep older adults mobile and independent for as long as possible.