Numerous studies have reported that driving cessation has negative impact on the well-being of older adults, such as depressive symptoms and physical, functional, and mental decline (Choi & DiNitto, 2015; Baldock et al., 2006; BoninGuillaume, 2010). The causes of driving cessation, including self-regulation, physical limitations, and functional mobility, are well-documented in scientific literature (Dickerson et al., 2007; Shaheen & Niemeier, 2001; Rosenbloom, 2012). However, strategies to delay driving cessation in older adult populations are lacking (Betz et al., 2014). This study describes characteristics of older adults who reported receiving rehabilitation specifically to improve their driving and other transportation use, based on the National Health and Aging Trends Study (NHATS). Among characteristics explored in this study, marital status was strongly associated with rehabilitation utilization to improve driving. Older adults who were living alone, single, separated or never married were the least likely to receive rehabilitation services to improve their driving in the past year compared with married older adults. Widows were less likely to receive rehabilitation services to improve their driving in the past year compared with married older adults (although the difference was not statistically significant).
Methods
This study used data from the National Health and Aging Trends Study (NHATS; www.nhats.org), a longitudinal cohort study that gathers information on a nationally representative sample of Medicare beneficiaries aged 65 and older across the country. NHATS currently consists of five rounds of data, starting in 2011 (round 1) to 2015 (round 5). Round 5 is the first round to address specifically the utilization of rehabilitation services among the sampled population. This study describes characteristics of older adults living in the community (i.e., not in a nursing home) who received rehabilitation services in the past year to improve driving or to improve the use of other forms of transportation or for other purposes besides transportation. Rehabilitation includes services such as physical therapy, occupational therapy, or speech therapy for various purposes. Information collected for this study also included demographic information, health status and physical function. Demographic information includes gender, age, race, education level, and marital status. Self-reported health conditions include heart attack, heart disease, high blood pressure, arthritis, osteoporosis, diabetes, lung disease, stroke and/or cancer. These were collapsed together to create a comorbidity count or the number of conditions a participant has (listed in Table 1). Dementia/Alzheimer’s disease and depressive symptoms were measured separately (Kasper et al., 2013; Choi & DiNitto, 2015). Using the Short Physical Performance Battery (standing balance, chair stands, and walking speed), the composite score was created to measure lower extremity physical function (Guralnik et al., 1994). NHATS’ weights were used to create a representative sample of the United States as well as to adjust for the complex sample design. The study first looks at the simple relationship between reasons for rehabilitation with other possible predictive variables using a Rao Scott Chi square test. In addition, a weighted multiple logistic regression model was conducted to evaluate demographic information, health status, and physical function as predictors of rehabilitation use to improve driving ability. Due to the weights, the model was fitted using Wald tests.
Results
Out of the 7,062 older adults in the NHATS round 5 cohort living in the community (and not in a nursing home), 19% (n=1,335) reported using rehabilitation in the past year.
Table 1 shows that of these 1,335 individuals, 10% (n=128) reported using rehabilitation specifically to improve driving ability, while 2% (n=25) reported using rehabilitation to improve ability in using other transportation modes. Marital status was found to be associated with rehabilitation use between three different rehabilitation categories (Table 1). Although not statistically significant, the peak years for receiving rehabilitation for driving ability appear to be between 65- 79 (ranging from 21-35%) with utilization decreasing more than half after the age of 80 (range 3-11%) (Table 1).
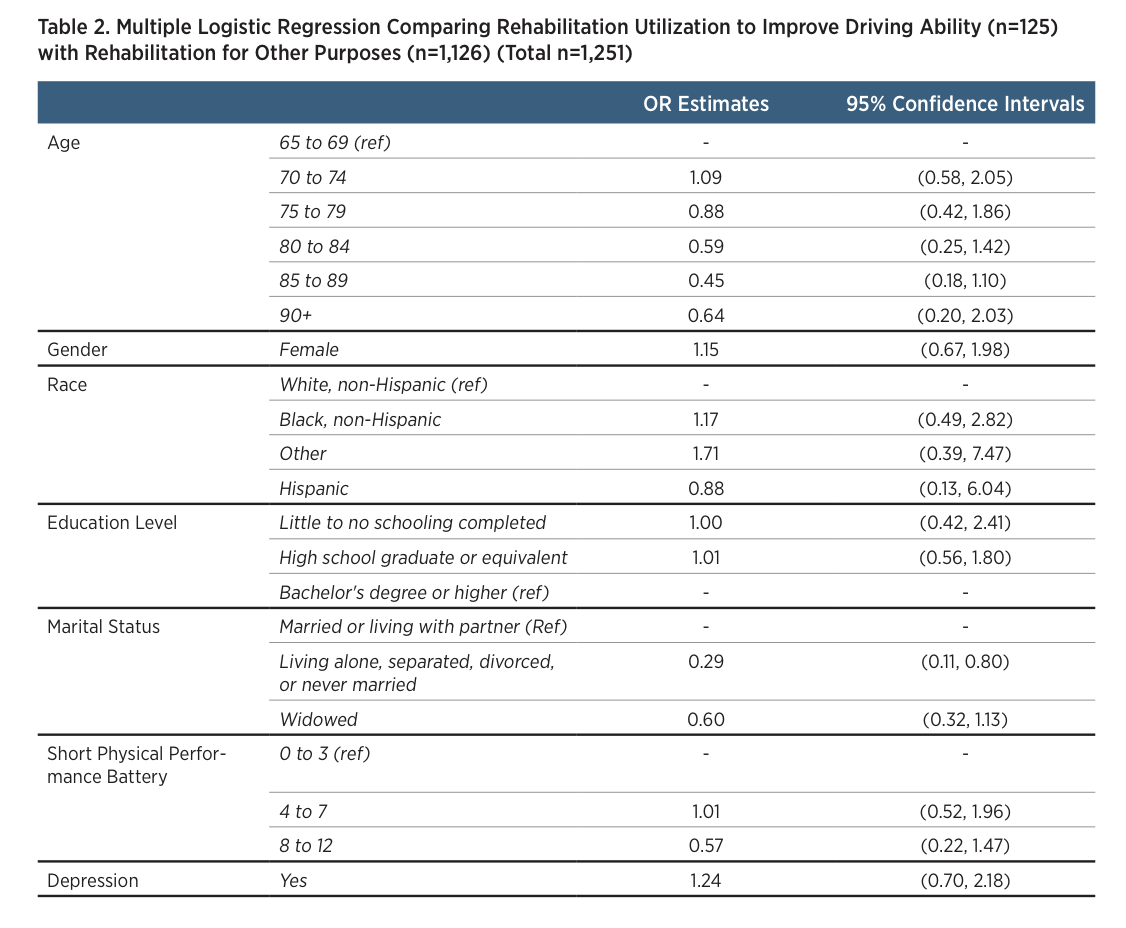
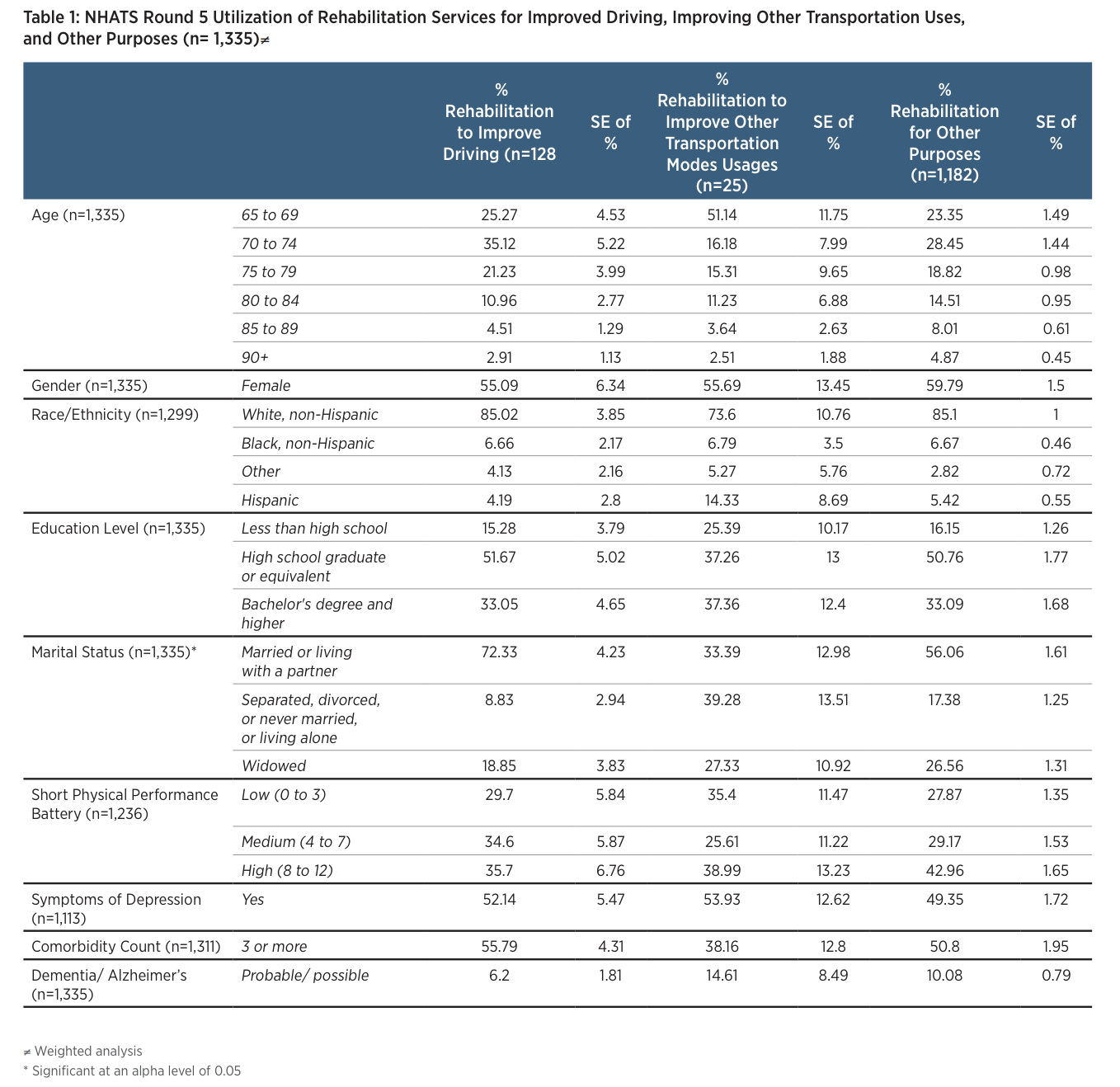 Table 2
Table 2 shows the results of the weighted multiple logistic regression, modelling utilization of rehabilitation to improve driving ability over other reasons for rehabilitation with demographic characteristics, health characteristics, and physical function. Dementia/ Alzheimer’s and comorbidity count did not contribute significantly to the model and were dropped. After controlling for other factors, older adults who were single, separated, or never married were less likely to use rehabilitation for improving driving ability, compared to older adults who were married (OR: 0.29; 95% CI: 0.11 – 0.80). Although a significant association was not established, older adults who were widowed were less likely to use rehabilitation services to improve driving ability compared with older adults who were married (OR: 0.60; 95% CI: 0.32-1.13). In addition, trends show that participants who had better lower extremity physical functioning (measured by the Short Physical Performance Battery) were less likely to report utilizing rehabilitation services to improve driving ability
Discussion
Relative to married older adults, single (includes never married and separated) older adults were the least likely to utilize rehabilitative services to improve driving ability. In addition, relative to married older adults, widows were less likely to report utilizing rehabilitation services specifically to improve driving, although this finding was non-significant, perhaps due to small sample sizes. Single older adults might benefit from targeted evaluation for driving rehabilitation. When older adults lose their spouses, it may be an important time to evaluate driving rehabilitation, since driving provides adults with a means to engage in a social network and to maintain their independence.
Older adults who are no longer able to drive may rely on other types of transportation such as using the bus, taking a cab, or other forms of public transportation (Cvitkovich & Wister, 2001; Davey, 2007; Levasseur, 2015). The sample size for looking at improving other types of transportation was too small (i.e., n=25 in Table 1) to derive any technical conclusions. However, rehabilitation in improving the use of other transportation modes may further play a role in maintaining the independence of older adults and will be important to research in larger samples.
The NHATS cohort provides a unique opportunity to explore rehabilitation utilization in a nationally representative sample of older adults. Over time, we may be able to study the association of driving related rehabilitation with driving cessation and its outcomes. However, since this is the first round of NHATS that collected information on rehabilitation, information on how long participants received rehabilitation prior to data collection is unknown. It is also difficult to determine the relationship between the characteristics described in the study and how long before rehabilitation is utilized to improve driving.
As our population continues to age, it is important that we explore ways to allow older adults to maintain their independence. Driving provides a means of independence, and rehabilitation to improve driving ability may play a role in keeping older adults mobile.
References
Baldock, M. R. J., Mathias, J. L., McLean, A. J., & Berndt, A. (2006). Self-regulation of driving and its relationship to driving ability among older adults. Accident Analysis & Prevention, 38(5), 1038-1045.
Betz, M. E., Dickerson, A., Coolman, T., Schold Davis, E., Jones, J., & Schwartz, R. (2014). Driving rehabilitation programs for older drivers in the United States. Occupational therapy in health care, 28(3), 306-317.
Bonin-Guillaume, S. (2010). Elderly drivers: Assessing performance or predicting driving safety. European Geriatric Medicine, 1(2), 93-94.
Choi, N. G., & DiNitto, D. M. (2015). Depressive symptoms among older adults who do not drive: association with mobility resources and perceived transportation barriers. The Gerontologist, gnu116.
Cvitkovich, Y., & Wister, A. (2001). The importance of transportation and prioritization of environmental needs to sustain well-being among older adults. Environment and Behavior, 33(6), 809-829.
Davey, J. A. (2007). Older people and transport: coping without a car. Ageing & Society, 27(1), 49-65.
Dickerson, A. E., Molnar, L. J., Eby, D. W., Adler, G., Bedard, M., Berg-Weger, M., & Page, O. (2007). Transportation and aging: A research agenda for advancing safe mobility. The Gerontologist, 47(5), 578-590.
Gell NM, Mroz TM, Patel KV. (2017). Rehabilitation Services Use and Patient Reported Outcomes among Older Adults in the United States, Archives of Physical Medicine and Rehabilitation doi: 10.1016/j. apmr.2017.02.027.
Guralnik, J. M., Simonsick, E. M., Ferrucci, L., Glynn, R. J., Berkman, L. F., Blazer, D. G., Scherr, P.A., &Wallace, R. B. (1994). A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. Journal of Gerontology, 49(2), M85-M94.doi: 10.1093/geronj/49.2.m85
Kasper, Judith D., Freedman, Vicki A., and Spillman, Brenda. (2013). Classification of Persons by Dementia Status in the National Health and Aging Trends Study. Technical Paper #5. Baltimore: Johns Hopkins University School of Public Health. Available at www.NHATS.org.
Levasseur, M., Généreux, M., Bruneau, J. F., Vanasse, A., Chabot, É., Beaulac, C., & Bédard, M. M. (2015). Importance of proximity to resources, social support, transportation and neighborhood security for mobility and social participation in older adults: results from a scoping study. BMC public health, 15(1), 503.
Rosenbloom, S. (2012). The travel and mobility needs of older people now and in the future. In J. F. Coughlin & L. A. D’Ambrosio (Eds.), Aging America and transportation: Personal choices and public policy (pp. 39-54). New York: Springer.